Health Plan administrative margins are shaped by more than reimbursement rates; price uplifts and labor costs. Equally important is how efficiently core operational workflows run across provider data, onboarding, directory maintenance, and contracting.
Many of the most persistent margin losses do not begin as major operational failures. They begin as manual intake steps, delayed updates, multiple reviews, and repeated reconciliation across disconnected systems. Over time, those small inefficiencies accumulate into slower onboarding, higher administrative cost, rework, and weaker financial predictability.
That compounding effect of small inefficiencies building into larger operational drag is not confined to one workflow. The 2024 CAQH Index estimates that the industry, which already avoids $222 billion annually through existing automation, could unlock another $20 billion in annual savings by moving more administrative processes from manual to electronic workflows. It also identifies eligibility and benefit verification and claim status inquiries as the two largest remaining savings opportunities, together representing more than $15 billion in annual potential savings. For payer operations leaders, this reframes manual workflow design from an operational concern to a strategic margin lever.
Also Read | Provider Data Management: A Strategic Guide for Health Plans
Where Manual Workflows Put Margins Under Pressure
Manual workflows rarely stay contained within one team. In payer operations, they tend to create friction at the point of intake and then push that friction downstream into adjacent functions.
Fragmented Intake Creates Avoidable Rework
A provider roster arrives in a non-standard format. Teams reformat it, check attributes against business rules, flag exceptions, reconcile records against internal systems, and follow up on items that do not process cleanly. What looks like routine processing is often a chain of preventable handoffs.
Delayed Updates Affect More Than One Workflow
The cost does not sit only in labor. Delays in updating provider information affect onboarding, provider directories, and downstream processing. Errors introduced upstream then create additional review and correction work later in the cycle.
Human Dependency Hides Structural Inefficiency
This is why manual workflows remain a margin problem even when organizations are used to them. Teams absorb the friction, staff around it, and eventually treat it as normal operating overhead instead of a structural workflow design issue.
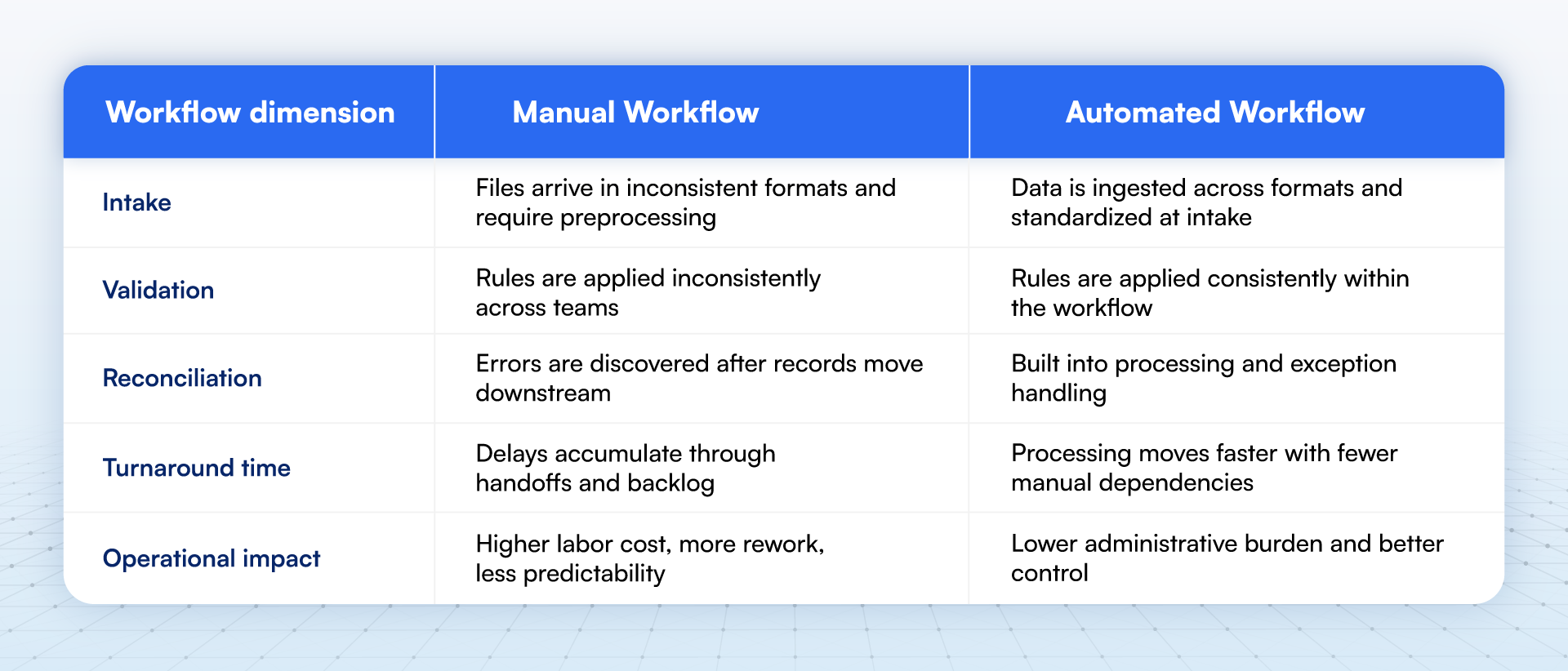
Manual vs. Automated Workflows: What Actually Changes
The real distinction is not between people and technology. It is between workflows that depend on repeated manual correction and workflows that apply structure early enough to prevent that correction from becoming necessary.
This distinction is especially visible in provider data operations. HiLabs MCheck® Roster Automation ingests roster files in any format, standardizing 300+ provider data elements, and applying configurable business rules across complex submissions, reducing roster turnaround time from more than 21 days to under 48 hours for a national Blue plan.
The Financial Impact Is Larger Than It Seems
The hidden cost of manual work is not just labor. It is the combined effect of rework, delay, unreliable execution, and exception handling across connected processes. When one workflow slows down, adjacent workflows inherit the cost.
In provider data operations, that pattern is easy to miss because the damage is distributed. A delayed roster slows provider onboarding. A late directory update increases member friction and service follow-up. A mismatch between source data and downstream systems creates exception handling. A manual rules processing becomes harder to sustain as markets, delegated entities, and submission formats diversify.
The compliance dimension makes the margin impact more concrete. Under 29 U.S.C. § 1185i, plans and issuers must verify provider directory information at least every 90 days and update the online directory within 2 business days of receiving updated provider-submitted information. When updates depend on slow, fragmented workflows, administrative drag becomes compliance exposure.
The data-quality problem is also well documented. A recent JAMA study examining physician directory entries across five large national insurers found directory inconsistencies for 81% of physicians. Those inconsistencies were driven largely by address discrepancies affecting 72% of physicians and specialty inconsistencies affecting 32%. For health plans, those are not abstract data-quality issues. They indicate workflow environments where teams must repeatedly validate, reconcile, and correct information before it can be trusted operationally.
That is why provider data processing costs a lot more to the health plans, hence impacting margin. When intake, validation, and update workflows improve, the benefit is not limited to one team. It affects onboarding speed, directory accuracy, downstream processing quality, and the amount of manual intervention required to keep operations moving.
What Better Execution Looks Like in Practice
Organizations that improve these workflows usually do not start with sweeping transformation programs or high-level efficiency mandates. They start by tightening workflow design and reducing the number of points where teams must stop, interpret, correct, and rework the same information.
The first shift is structural. High-performing organizations define ownership at each stage of intake, validation, data standardization, and update. That matters because manual workflows often fail in the gaps between teams, not only within teams. When ownership is diffused, data quality is sub-optimal and non-standardized; data issues sit longer, exceptions multiply, and turnaround times become harder to control.
The second shift is temporal. Better-performing teams standardize data earlier and validate data on an ongoing basis. They do not rely on periodic cleanup to catch issues that should have been resolved closer to intake. In provider directory operations, that matters because federal rules require ongoing verification and fast updates once new information is received.
The third shift is operational. Approved changes must propagate across dependent systems instead of stopping at the first update point. When that does not happen, downstream teams end up reconciling records manually, service teams absorb the fallout, and the organization pays significantly higher for the same data problem.
Read More | How Leading Health Plans Improve Provider Data Accuracy and Lower Cost of Care
How Health Plans Can Reduce Manual Workflow Burden Across Provider Data Operations
Reducing manual workflow burden starts with identifying where teams spend time correcting, reformatting, validating, and reprocessing the same data across systems.
Roster Processing
For many health plans, provider roster processing is one of the clearest examples. Files arrive in different formats; business rules vary across markets and lines of business, and updates often require multiple rounds of review before they can be applied. That slows provider onboarding, increases operational cost, and creates backlog risk.
HiLabs Roster Automation is built for this part of the workflow. It helps health plans to ingest roster files in different formats, standardize provider data, apply configurable business rules, and support reconciliation within a governed, AI rules-based workflow.
Explore MCheck® Roster Automation →
Directory Maintenance
For health plans, directory maintenance and validation present a related challenge. Even after provider data is loaded, it must be validated and kept current. When plans rely on manual outreach, provider attestations, or periodic cleanup cycles, inaccuracies can persist longer than they should. That creates member friction and increases compliance exposure.
HiLabs Provider Data Accuracy (PDA) addresses this problem by helping plans validate and enrich provider data across thousands of sources, scoring updates for reliability, relevance, and recency. Instead of relying only on periodic manual review, plans can take a more systematic approach to maintaining directory accuracy.
Explore MCheck® Directory Accuracy →
Contracts Management
Manual workflow pressure also extends beyond provider data. In payer-provider contracting, teams often work through fragmented documents, slow review cycles, and labor-intensive pricing configuration. That creates another layer of delay and operational dependence on a small group of specialists.
HiLabs ContractsAI addresses these workflows by helping plans analyze contract language, support pricing configuration, and improve access to contract intelligence across the contract lifecycle. While contracting is a different operational domain, the underlying issue is similar: manual, fragmented processes create avoidable delay, cost, and risk.
Across these areas, the broader pattern is consistent. The more operational work depends on manual intake, repeated review, and downstream correction, the harder it becomes to improve speed, accuracy, and margin performance. That is why the business case for workflow redesign is stronger than a simple labor-savings argument. Better workflow design can reduce avoidable administrative effort, lower the volume of exceptions, and shorten the lag between receiving new information and making it usable across the organization. The CAQH Index makes that broader point at industry scale: substantial savings remain available where manual administrative work still dominates.
Conclusion
Manual workflows weaken operating margins for health plans in ways that are easy to normalize and hard to isolate. The cost rarely sits in one broken process. It spreads across intake, validation, reconciliation, downstream correction, and delayed execution.
For health plans, provider data operations make that pattern especially visible. When provider information moves slowly, arrives in inconsistent formats, or requires repeated manual review; the impact shows in onboarding delays, directory inaccuracy, compliance risk, and added administrative burden. The JAMA findings on health plan directory inconsistencies and the federal provider-directory update requirements both reinforce the same point: weak provider-data workflows create operating and regulatory consequences at the same time.
That is why better performance usually starts with workflow structure, not with abstract calls for efficiency. Standardizing earlier, validating more continuously, and reducing downstream correction can make provider-data operations more reliable and more scalable. In an environment where billions in administrative savings remain unrealized, workflow quality is not a background operational detail. It is a margin lever.
